- 1. Background
- 2. Abnormality Detection (Lesion Segmentation)
- 3. Neural Substrate
- 4. Outcome Prediction
- 5. References
1. Background. Neonatal brain injury caused by hypoxic ischemic encephalopathy (HIE) affects 1-5/1000 term-born infants. Therapeutic hypothermia (TH) reduces mortality/morbidity by cooling patients to 33-34°C for 72 hours. Nevertheless, many patients still die or suffer lifelong disabilities. One path to improve HIE outcome is to further improve neonatal treatment, but the progress is slow because outcomes are hard to assess until 18-24 months old (Fig 1C). Another path is to early intervene, which requires us to identify at-risk patients ideally during the neonatal stage (Fig 1A). Both paths are blocked by the same problem -- an unmet need for methos that can accurately identify brain abnormalities/lesions associated HIE, and predict 18-24-month neurocognitive outcomes in the neonatal stage.
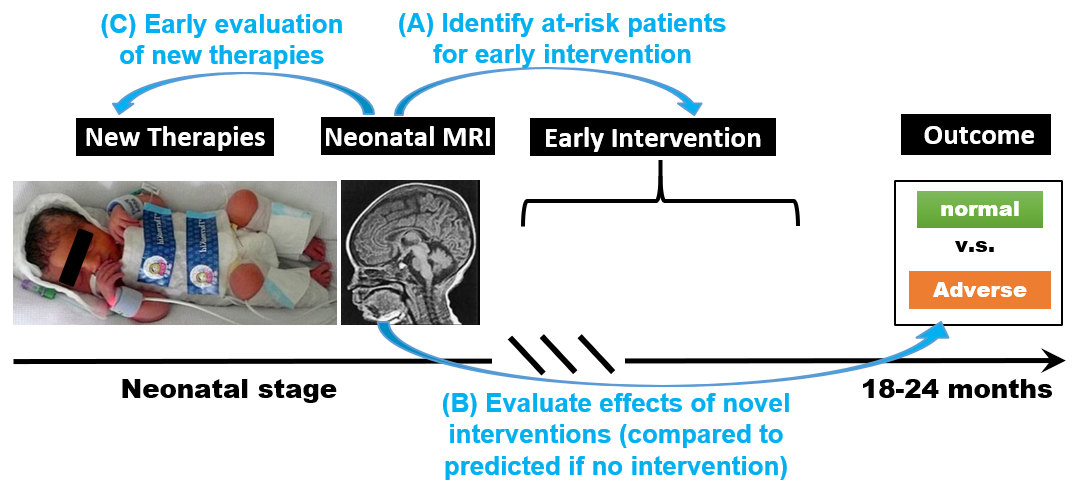
Fig 1. Unmet need in HIE for abnormality detection and outcome prediction.
Neonatal brain MRI is being explored to identify HIE lesions and predict HIE outcomes, due to its non-invasiveness, its being routinely acquired for HIE care, and its potential to show 3D injury patterns [Weiss_Bates_2019]. However, MRI is currently only interpreted by experts, subject to 20-40% uncertainty and unsatisfactory accuracy. We develop sophisticated algorithms for
- (i) detecting HIE lesions;
- (ii) quantifying neural substrate of outcomes; and
- (iii) predicting HIE outcomes.
2. Abnormality Detection (HIE lesion segmentation). HIE lesions are often diffuse (multi-focal). Experts often rely on apparent diffusion coefficient (ADC) maps for lesion detection. Abnormally low ADC values -- corresponding to restricted water/blood flow -- usually show signs of lesions. However, identifying abnormally low ADC values can be challenging (Fig 2). A fundamental dilemma is: how low an ADC value is too low, and how low is within the normal range of variations?

Fig 2. Finding brain regions with abnormally low ADC values can sometimes be very challenging.
We developed normal neonatal brain ADC atlases [Ou2017; Sotardi2021], which quantified voxel-wise normal ranges of ADC variations. We further developed algorithms that convert each ADC map into a ZADC map, which quantified voxel-wise deviation from normal [Pinto2018; Zhang2021a] (Fig 3).

Fig 3. Concept of ADC atlas and ZADC map.
Technically, explicitly adding anatomy information into deep learning convolutional neural networks (CNNs) has shown promise to improve the accuracy of segmenting small and diffuse brain lesions [Zhang2021b]. Our atlas and ZADC map push this concept one step further -- not only anatomic location matters, more importantly, the normal variations and deviation from normal at each anatomic location matter. Results are promising. We show that [Zhang2021a]
- ZADC map could significantly improve the HIE lesion segmentation accuracy compared to using ADC maps (Fig 4, fourth and fifth columns);
- combing ADC and ZADC maps achieved an even higher accuracy than ZADC map alone (Fig 4, fifth and sixth columns);
- moreover, the accuracy is equivalent for data acquired in GE 1.5T scanner and data acquired in Siemens 3T scanner (Fig 5).

Fig 4. HIE lesion segmentation by deep learning, contrasting between using ADC map and ZADC maps.

Fig 5. Generality across scanners.
3. Neural Substrate. Neural substrate refers to neuroanatomic factors underlying or correlated with outcomes. Currently, NICHD Neonatal Research Network (NRN) scoring system is the norm to evaluate HIE severity in MRI and to predict outcome. NRN scores (Fig 6) assumes that
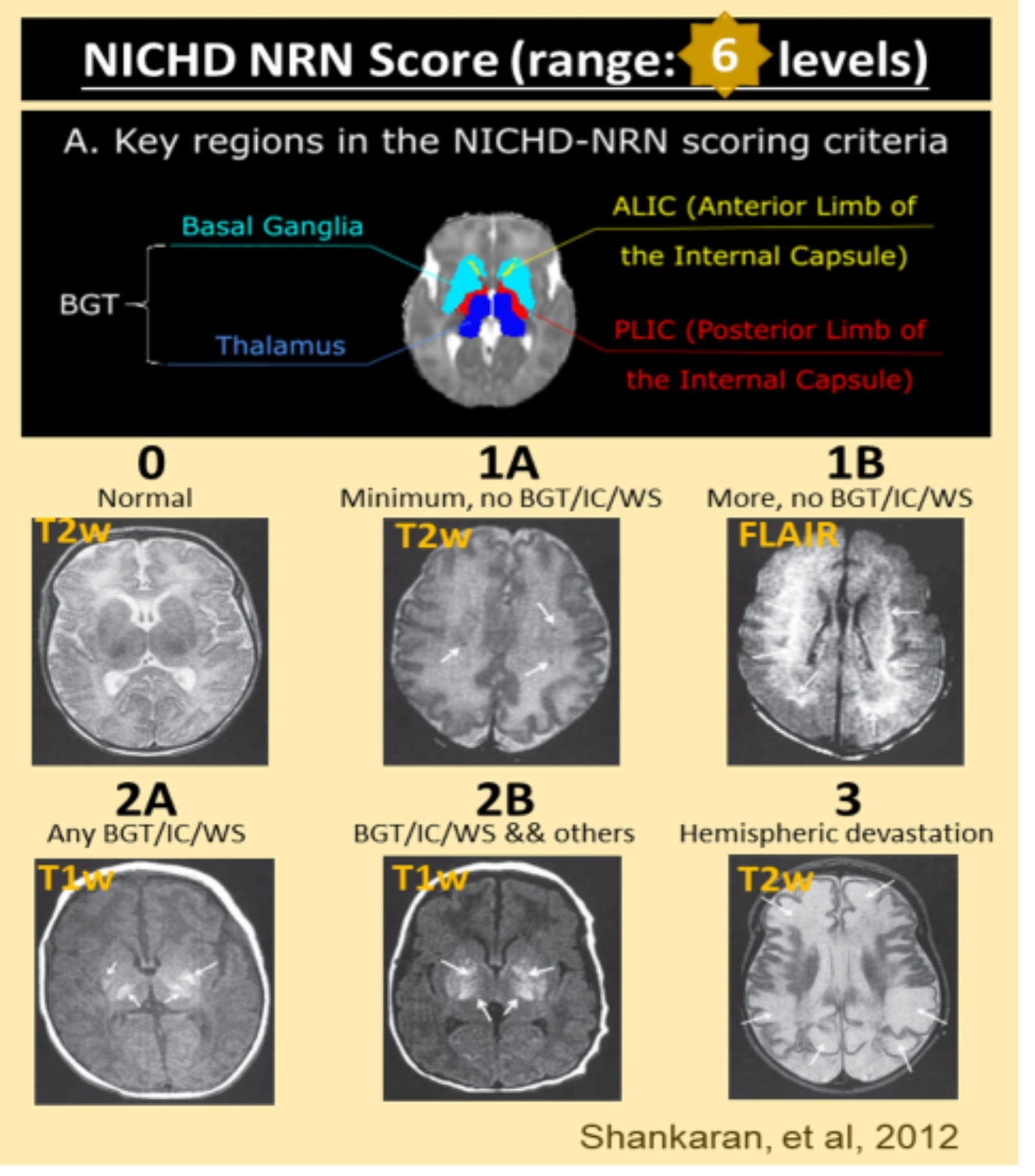
Fig 6. NICHD Neonatal Research Network (NRN) scoring system. It focuses on certain anatomic regions.
Quantitative lesion-symptom mapping allows us to identify neural substrate at the voxel-, regional-, fiber-bundle level, and rigorously study hemispheric asymmetry in the brain involvement in the HIE outcome. We have found that (i)
4. Outcome Prediction. Outcome
5. References
[Weiss_Bates_2019] RJ Weiss*, SV Bates*, Y Song, Y Zhang, EM Herzberg, YC Chen, M Gong, I Chien, L Zhang, SN Murphy, RL Gollub, PE Grant†, Y Ou†, "Mining multi-site clinical data to develop machine learning MRI biomarkers: application to neonatal hypoxic ischemic encephalopathy", Journal of Translational Medicine, 17:385, (2019)
[Ou2017] Y Ou, L Zöllei, K Retzepi, V Castro, SV Bates, S Pieper, KP Andriole, SN Murphy, RL Gollub, PE Grant, "Using Clinically-Acquired MRI to Construct Age-Specific ADC Atlases: Quantifying Spatiotemporal ADC Changes from Birth to 6 Years Old", Human Brain Mapping, 38(6): 3052-3068, (2017).
[Sotardi2021] S Sotardi, RL Gollub, SV Bates, R Weiss, SN Murphy, PE Grant, Y Ou, "Voxel-wise and Regional Brain Apparent Diffusion Coefficient Changes on MRI from Birth to 6 Years of Age", Radiology, 298(2): 415-424, (2021).
[Pinto2018] ALR Pinto, Y Ou, M Sahin, PE Grant, "Quantitative Apparent Diffusion Coefficient Mapping May Predict Seizure Onset in Children With Sturge-Weber Syndrome", Pediatric Neurology, 84: 32-38, (2018).
[Zhang2021a] Y Zhang, S He, Y Song, SV Bates, RJ Weiss, C Jaimes Cobos, S Sotardi, SN Murphy, RL Gollub, PE Grant, Y Ou, "Quantifying location-specific normal variations improves deep learning segmentation of diffuse lesions: Demonstration in neonatal encephalopathy", under review, (2021).
[Zhang2021b] Y Zhang*, S He*, PE Grant, Y Ou, "Deep learning segmentation of small diffuse brain lesions: challenges, algorithms, and big data opportunities", under review, (2021).
[Song2021] under review (2021).